
Sarah Sample-Eppinger, DPM
Sarah Sample-Eppinger, DPM, a surgical podiatrist specialized in wound care and limb preservation, recently participated in a webinar to showcase a podiatry patient case with necrotizing soft tissue infection who was treated with RECELL® Spray-On Skin™ Cells, along with two other cases presenting with gas gangrene and necrotizing fasciitis.
The following is a shortened transcript of the discussion, including her view of RECELL as a point-of-care device in the operating room, and how it has transformed her standard of care.
If you prefer to watch the full recorded webinar, you can view it here.
Case study: RECELL for a complicated necrotizing soft tissue infection wound
Moderator: Let’s jump right into this case of yours that you shared of a 57-year-old female. Tell us about this complicated wound, what made you consider the use of RECELL, and why it ended up being a great situation for this patient.
Dr. Eppinger: This case is a great case from Dr. Ritter in New York, but this is the kind of patient that I see and this is an everyday occurrence in my practice.
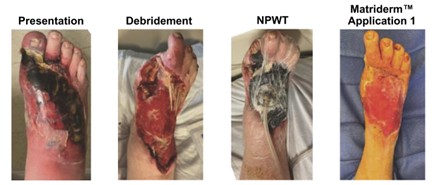
This is a patient that has multiple comorbidities, type 2 diabetes, coronary artery disease, who presents with a necrotizing soft tissue infection of the top of their foot. They initially are converted to clean with debridement, usually treated with negative pressure wound therapy, skin substitutes, all sorts of different products to get the wound to the point that it’s ready for split-thickness skin grafting, which is what you see on this page.

Once the patient’s foot has been converted to a clean, healthy, granular, bleeding wound-base, the patient’s ready for split-thickness skin grafting to finish getting them over the finish line. So you, in this case, use RECELL with the split thickness skin grafting because it helps decrease the amount of time it takes for the skin grafts to heal, decreases their likelihood of getting another infection, which is important in these really sick patients. And it decreases the amount of skin that has to be harvested, which is a really big deal, because we know that these patients don’t just have issues healing their feet, they have issues healing everything.

So this patient, you can see it 20 weeks post-op, has almost no contractures going on, which is a really big deal because those deformities that happen with the toes can cause additional ulceration in the future. And here she is back to walking and hiking and doing what she wants to do with her family in a much shorter timeframe than what existed before RECELL was available.
How RECELL has transformed her standard of care
Moderator: What are some of the other details that would be positive for people to understand about the RECELL System?
Dr. Eppinger: Things that I like about it: It has potential for cost savings because it decreases length of stay on in-patients. And because it decreases the amount of healing and time it takes for the harvest site because it is smaller, as well as for the actual site that you’ve grafted.
The other things that it does is it has less scarring because you’re getting those fibroblasts active in the interspaces in the split thickness skin graft spot, which decreases the need for additional surgical procedures like tendon lengthening, scar tissue revision.
And it also decreases the donor site pain because the smaller a donor site is, the less it hurts and the faster it heals. And the smaller a donor site is, especially for me as a podiatrist, is a really big deal because most of my patients are not healthy. Most of my patient are sick, their donor site is painful, it’s the only thing that hurts because of their neuropathy usually. When we decrease the amount of skin that we need to take, it increases the options for where you can take skin, which is important because not all podiatrists are fortunate… we can’t all harvest from thigh. Some of us have to harvest from below the knee. And it makes it so that wounds that are larger are more accessible for split thickness skin grafting.
RECELL as a point-of-care device in the operating room
Moderator: Can you tell us a little more about the RECELL System as a point-of-care device in the operating room?
Dr. Eppinger: Yeah, so there’s this box that we have these cartridges. The cartridge is what the skin goes into. (It) takes about 35 minutes for us to get the skin from skin coming off the patient to spray in your hand. It uses the natural regenerative capacity of the epidermis. It’s nothing from a box that goes on the patient. It’s the patient’s own skin that we use to help them heal. And it significantly reduces the amount of donor skin you need to take. Every one square centimeter of skin can cover up to 80 square centimeters of covered area.
Clinical evidence on RECELL
Moderator: Can you talk a little bit about the proven clinical safety and effectiveness of the RECELL system?
Dr. Eppinger: Absolutely. There have been several studies, and one of the things that I like about RECELL and about AVITA is that they didn’t just come up with this idea and throw it at you and say, “we’ll see how it works.” There’s actual clinical evidence for its use in partial thickness burns, for its used in mixed-depth burns, in full thickness skin defects that are non-thermal, and then also in vitiligo. And there’s a very robust and growing body of literature that exists that proves that this works. It’s not your usual product that they have one or two studies and they say, hey, this worked, they actually have a lot of good evidence behind it that shows efficacy.
Case study: RECELL for a gas gangrene wound
Moderator: Let’s show some of your cases that are specific to you and what things stood out for effectiveness on your treatment and plan with these patients.
Dr. Eppinger: Absolutely. So this is a 51 year old female who showed up in the emergency department with sepsis and with a gas gangrene picture going on. The initial incision and drainage was actually done by my colleagues in vascular surgery. They got the initial source control that they needed. That’s the first couple of pictures that you see. And then this is usually where they call us for aid. And they say, we’ve gotten rid of the bad stuff that’s making this patient sick. Can you please help us make it into a functional extremity?

She had very uncontrolled type 2 diabetes. She quit smoking the day she was in the hospital is what she told me. Had mild peripheral arterial disease. Her hemoglobin A1C on presentation was over 11. So she was very poorly controlled type 2 diabetic.
She got converted to a transmenotarsal amputation but due to the severity of the infection she did have some skin loss that was partial and full thickness. We applied some wound matrix over those areas once she was converted clean to promote healing and get us to a wound base that was gonna be graftable.
About 37 days after the bilayer wound matrix went on, we have this very nice granular appearing wound bed. This is how she appeared on the day of her procedure. I made the decision in this patient because it’s plantar skin to make my cell suspension out of plantar skin instead of out of skin from her thigh or her lower leg. One of the things that we are taught as podiatrists is split thickness skin grafting on the bottom of the foot isn’t successful because it’s not durable and it re-ulcerates because that skin isn’t designed to be walked on. One of the things that really excites me about RECELL is that it gives me the ability to create a graft that’s actually the patient’s. Not only their own skin but it’s also the right skin for the surface that I’m trying to treat.

So here she is on post-op day six. You can see that area towards the lateral side of the foot where that pass for the RECELL harvest was done, as well as the wounds that we were treating with the split thickness skin graft. I used a three-to-one mesh on that.
Then here she is post-op day 12. Post-op, day 28, it’s completely healed. It’s already starting to pigment. We cleared her to walk at post-up day 28. That’s unheard of for pretty much any other technology that exists. You’re not gonna see that with skin substitutes because they just don’t work the way that the patient’s own skin works.
When I harvest from plantar skin, I do two passes. So I do a first pass at a 0.020 inches depth. I save that to put back over the site where I’ve done the harvest. I take a second pass for the harvest at 0.008. That’s the piece that goes in the RECELL machine. And then the initial pass goes back over that site and gets sutured down with Monocryl™ to protect the site where the harvest was taken from.
Case study: RECELL for a necrotizing fasciitis surgical wound
Moderator: Thanks for sharing that great case with us. I think just seeing the patient’s comorbidities explains so much for the type of population of patients that you see within the surgical podiatry world. Let’s move on to the next one here. It’s a necrotizing soft tissue infection. Tell us about this one.
Dr. Eppinger: This is a very nice 45-year-old female who presented to my hospital system with true blue necrotizing fasciitis. She declined surgical intervention at presentation because she was worried about time down and about significant bleeding in the OR.
About hospital day five, she started to blister and it became very apparent that she wasn’t going to be able to avoid surgical intervention. And she finally agreed to it, but she had a large defect on the dorsal aspect of the foot from the tissue loss. With these necrotizing soft tissue infections, sometimes patients have delayed presentation for lots of reasons. And the longer that we delay getting them to the operating room, the more tissue loss you have. So in this case, it’s a very large tissue defect.
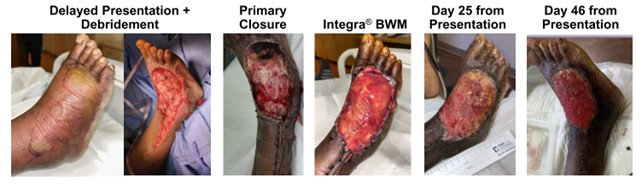
Once we had her converted to clean, we managed to primarily close part of the area, but not the entirety of it. And then applied a bilayer wound matrix again to help protect those tendons that you can see that are slightly exposed.
Day 25 from presentation, it’s looking much healthier. It’s improved some. You can still see some graft in that wound base. It wasn’t ready for skin grafting yet. And at day 46, she looked pretty ready to go for split-thickness skin grafting.
We made the decision to do RECELL on this patient and mesh her at a six to one, because one of her biggest concerns was she had a small child at home. She was trying to figure out how, with her one-year-old, she was going to feed them and do what she needed to do if she had large, harvest site on her thigh that was painful. So we did a six-to-one mesh, which enabled me to take significantly less skin from her thigh and helped alleviate her concerns about taking care of her family. We made the RECELL skin suspension.

By post-op day 33, she just had a few patches of area that were open. If she’d had a desk job, I actually would have cleared her to go back to work at post-op day 33. She worked in environmental services, so we waited a little bit longer to return her to work and wanted to make sure it was completely healed. So post-up day 45 is when I cleared her to go back to work.
At post- up day 60, you can even see the skin has remodeled some. There are no contractures. She’s not getting the issues with the hammer toes or ankle stiffness that sometimes comes with doing split thickness skin grafting this close to the ankle joint. She had a really great outcome. And I’m always struck when I do RECELL for my patients with how much pigmentation they get back so quickly.
Looking for more like this? Read New Real-World Study Strengthens the Economic Case for RECELL.

About the author
Sarah Sample-Eppinger, DPM, is a doctor of podiatric medicine who works in wound care and specializes in podiatry, with a subspecialty in amputation prevention. Her area of focus is on wound care and limb salvage, as well as forefoot, rearfoot, and ankle surgery.
Dr. Sample-Eppinger collaborates with vascular surgeons to provide non-surgical treatment options and to prevent limb loss from vascular diseases. She received her CWSP© (Certificate of Wound Specialist Physician) from the American Board of Wound Management.
She earned her Doctor of Podiatric Medicine in 2016 from Des Moines University College of Podiatric Medicine and Surgery. Dr. Sample-Eppinger worked as a podiatrist and a medical director of a wound care department prior to joining Kettering Health.


